Post Prostatectomy Incontinence
What is post prostatectomy incontinence?
Despite improvements in surgical approaches, changes in urinary function inevitably occur after radical prostatectomy (RP). Stress urinary incontinence (SUI - leakage on coughing, sneezing or doing heavy physical work) is the most common type of urinary leakage after RP. A smaller proportion may get leakage because of an overactive or underactive bladder.
Risk factors that may predispose patients to develop SUI include
Age
Obesity (BMI >30)
Other medical problems such as neurological problems and pre-existing urinary problems
Anatomical factors such as prostate size and small urethral length
Complications of surgery such as urine leak and strictures
Experience of surgeon and surgical technique
SUI often resolves in approximately 90% within the first postoperative year. 5-10% of patients may require further surgery for ongoing SUI after 1 year.
How is post prostatectomy incontinence assessed?
Treatment depends on the extent of urinary leakage and degree of bother to the patient.
Thorough evaluation consists of a detailed history and physical examination. Leakage is quantified by the number of pads used per day and the weight of pads used over a 24-hour period. You may be asked to fill out questionnaires that assess how much the leakage is affecting your quality of life.
Further investigations may include:
Urine tests including checking for infection and general blood tests
Bladder diary to record how much and when urine is passed
Assessing the flow of your urine and volume left in the bladder after passing urine
Ultrasound of the bladder and kidneys to assess anatomy
Cystoscopy to assess your sphincter muscle and to exclude a stricture (scar tissue)
Urodynamics to assess function of your bladder - specifically this is always done when underactive or overactive bladder is suspected, the treatment of which differs to that of SUI.
What are the treatment options for post prostatectomy incontinence?
Treatment options for post prostatectomy incontinence include:
Conservative approaches (within first 12 months)
Lifestyle changes (reduce fluids, caffeine and alcohol and weight loss)
Pelvic floor physiotherapy exercises
Surgical approaches (for those who have problematic leakage beyond 12 months)
Male sling (Fig 1) – Adjustable and non-adjustable
Ideal for those with mild SUI
Not suitable for those with previous radiotherapy
Artificial urinary sphincter (Fig 2) – the gold-standard treatment and last resort
Ideal for those with severe SUI, previous radiotherapy or failed previous treatments

Figure 1. Male Post Prostatectomy Incontinence Sling
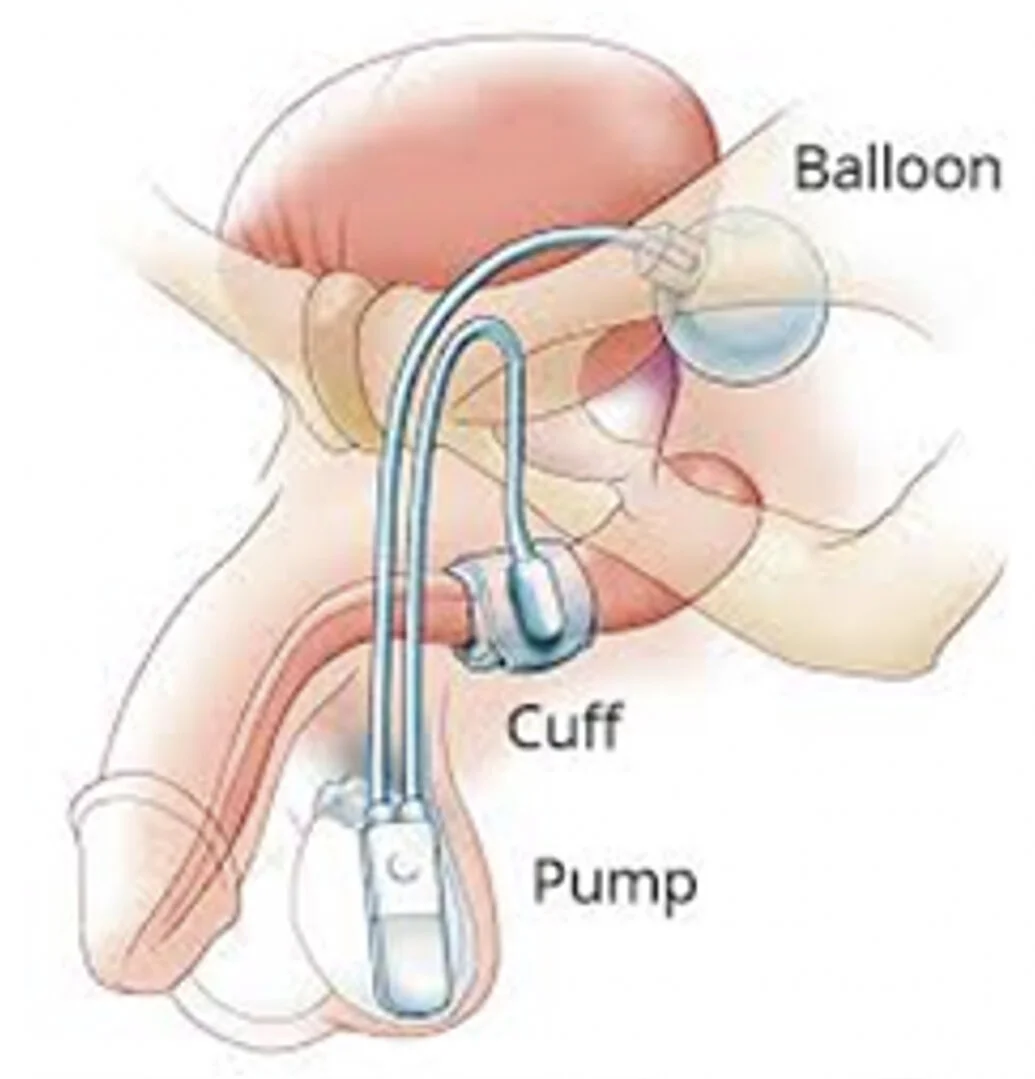
Figure 2. Artificial Urinary Sphincter