Prostatectomy - Open Radical

Figure 1: Incision for open radical prostatectomy.
What are the indications for a robotic radical prostatectomy?
An open radical prostatectomy is performed to treat prostate cancer.
What pre-operative work up is needed?
Your urologist will organise any necessary urine and blood tests and imaging scans at your consultation prior to your procedure. Your work-up will include a PSA test, an MRI scan of the prostate and prostate biopsy to confirm prostate cancer. Depending on the aggressiveness of your cancer, you may also need some staging scans such as PET scan (to check if the cancer has spread beyond your prostate gland to the bones or lymph nodes). You may need special tests and scans to assess your fitness for surgery.
If you take any blood thinning medication such as aspirin, warfarin, plavix (clopidogrel) or other anticoagulants, you should discuss with your urologist if these need to be stopped before your procedure.
You will see a pelvic floor physiotherapist who will teach you how to do your post-operative pelvic floor exercises prior to your surgery. You will also see a prostate cancer specialist nurse to discuss aspects of your care.
Please ensure you return any admission forms given to you to be filled out back to the hospital.
What happens on the day of the procedure?
You will be given fasting instructions prior to your admission (usually for 6 hours prior to the procedure). You should bring a list of your medications, any recent scans or reports with you to the hospital. After you are admitted from the admission lounge, your urologist will see you to discuss the surgery. An anaesthetist will see you to discuss the general anaesthetic and pain relief options before you are taken to the operation theatre. You will be provided with a pair of TED stockings to wear to prevent blood clots from developing and passing into your lungs.
What does this procedure involve?
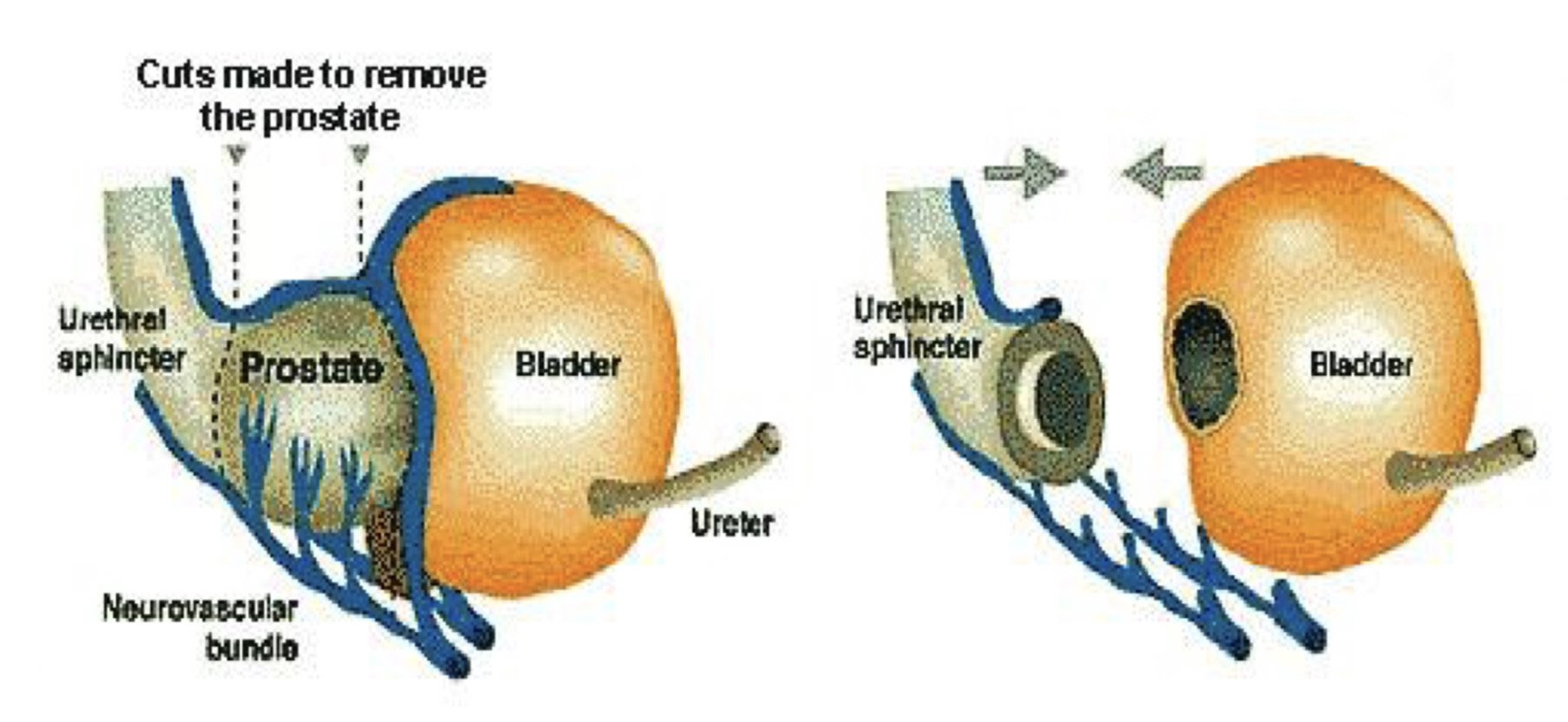
Figure 2: Radical Prostatectomy.
This involves very precise removal of the whole prostate gland, seminal vesicles and, sometimes, the draining lymph glands, as well as tying off the vasa deferentia (sperm-carrying tubes). It is performed through an 8-10cm cut in your lower abdomen.
The aim of the surgery is:
to remove the cancer;
to achieve a clear margin away from the tumour;
to drop the PSA blood level below 0.1 ng per ml;
to reduce the need for any further treatment (e.g. radiotherapy or hormone treatment);
to preserve your continence; and
if possible and appropriate, to preserve the nerves to your penis that control the ability to have an erection
After a full general anaesthetic and an injection of antibiotics before the procedure, a catheter is inserted into your bladder, during the operation. The operation is performed through a 10cm lower abdominal midline incision.
The surgeon will detach the prostate from the bladder and urethra (waterpipe) and rejoin the bladder to the urethra. The surgeon will aim to spare all the muscles and urethral fibres, which are vital for early return of continence. The nerves that are responsible for erections can be spared if appropriate to do so (sparing the nerves is only appropriate/possible if the cancer has not come closer to the layer in which they lie). The procedure usually takes three to four hours to perform. You will have a drain tube in your abdomen to remove any excess fluid. Any blood lost during the operation is collected in a cell saver and returned back to your body to reduce the chance of needing a blood transfusion of foreign blood.
After the procedure, you are given a fluid based diet that day. The next day, you will be given injections to thin your blood to prevent clots in the legs and lungs and encouraged to do deep breathing exercises and move around the ward. The drain is removed as soon as you are mobile and you are able to eat a normal diet. You will be in hospital for 3-4 days.
You will be taught how to manage your catheter (see catheter care information sheet) before you go home.
Are there any risks or side-effects?
Pain or discomfort at the incision site 50-80%
Temporary abdominal bloating (gaseous distension) 10-20%
Bleeding, infection, pain or hernia at the incision site requiring further treatment 2-3%
Bleeding during or after surgery requiring transfusion 5-10%
Tumour at the margin of resection requiring close observation or needing other treatments at a later date 15-20%
Injury to other organs (bowel, urine tubes)/blood vessels/nerves 1-2%
Persistent urine leak from the joint 3-5%
Scar tissue at the joint needing further surgery 3-5%
Temporary urinary leakage 70-100% (improves with time)
Long term urinary leakage needing further continence surgery 5-10%
Sexual dysfunction including loss of erections, penile shortening and dry orgasms 50-100% (improves with time)
Major anaesthetic or cardiovascular problems possibly requiring intensive care (including chest infection, pulmonary embolus, stroke, deep vein thrombosis, heart attack and death) 3-5%
What can I expect after discharge when I get home?
It will take 7-10 days to recover fully from the procedure. Most people can return to normal activities, and light work duties after 3-4 weeks and strenuous activity and driving after 6 weeks if you are comfortable and the GP is happy with your progress.
You will be discharged with a catheter and leg bag. You will be shown how to manage and empty this (see catheter care sheet). Drink plenty of water to keep your urine clear. You will receive an appointment for removal of catheter 10-14 days. You wound sutures are dissolvable and do not need removal.
Avoid straining on the toilet, which may put pressure on the internal joint. Laxatives and a high fibre diet will help.
Most men experience some leakage of urine on catheter removal. You should commence your pelvic floor exercises (see Pelvic Floor Exercises for Men information sheet) and the urinary leakage will improve with time. If you had a nerve sparing operation, you may be prescribed Sildenafil (Viagra) to maintain blood flow to your penis. Your urologist and prostate cancer nurse will explain how you can enjoy a healthy sex life after surgery, even if the nerves do not recover or need to be removed.
If you feel unwell, have a fever, difficulty passing urine or redness or discharge from your wound, you should contact your GP to check for a urine infection or come to the ED.
What follow-up will I require?
You will receive an appointment for removal of catheter in 14 days if there are no concerns with the joint. In some cases the surgeon may request an X-ray to check that the joint has healed sufficiently before removing the catheter. You will see the urologist at 2-3 weeks around the time of your catheter removal. You will have your first PSA check and appointment 2 months after the procedure then periodically thereafter for 3-5 years.