Penile Straightening
What are the indications for a penile straightening?
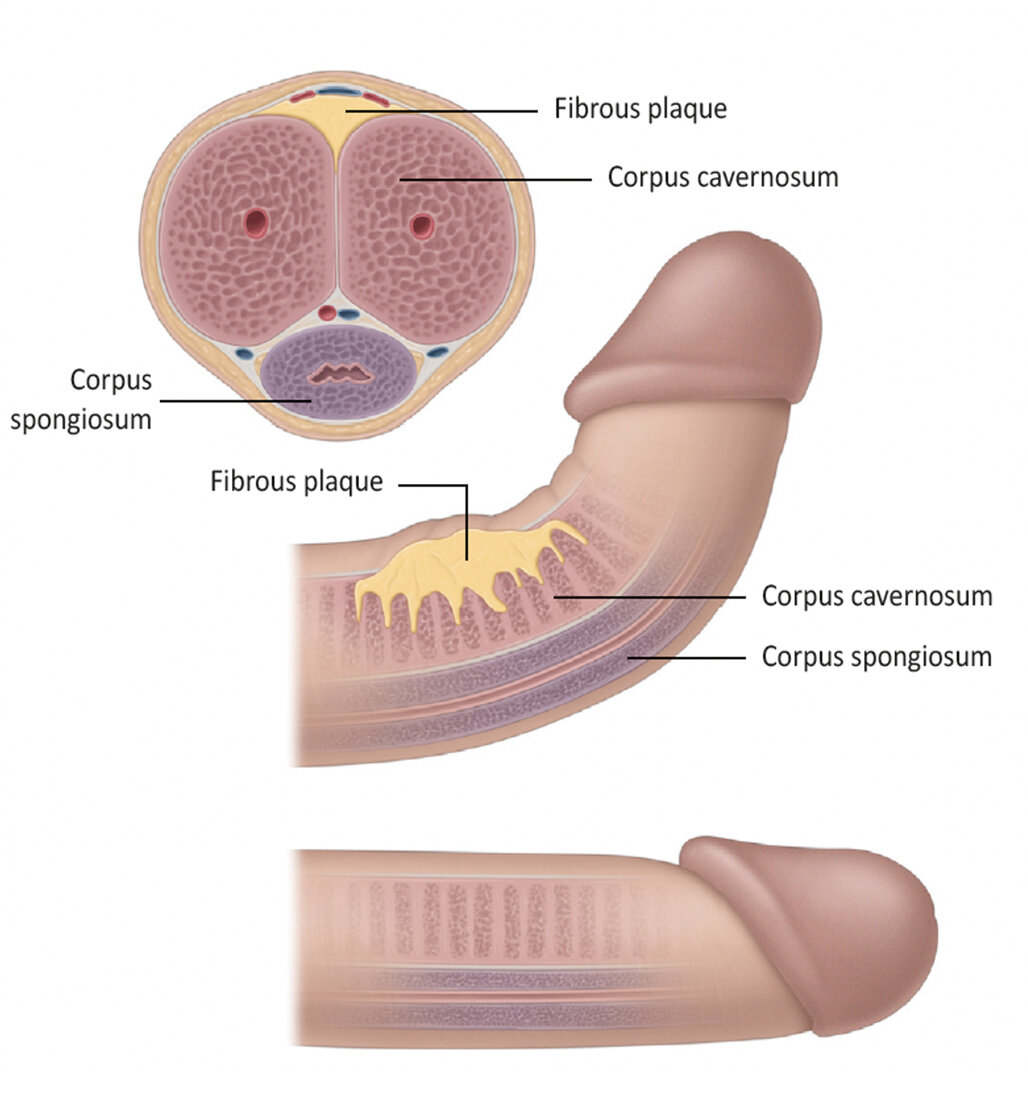
Figure 1. Penile curvature.
Penile plication is indicated in patients with a penile curvature angle greater than 30° associated with difficulty in vaginal penetration in patients who are able to achieve an erection.
Your urologist will wait until your peyronie’s disease has reached a stable phase (no pain or worsening of curvature for 3-6 months) before recommending surgical treatment.
What pre-operative work up is needed?
Once your urologist has established a diagnosis by history and either photos or erections or an artificial erection test, in most cases, no significant work-up is needed. Your urologist will organise any necessary urine and blood tests at your consultation prior to your procedure.
If you take any blood thinning medication such as aspirin, warfarin, plavix (clopidogrel) and anticoagulants, you should discuss this with your urologist, as they may need to be stopped temporarily.
Please ensure you return any admission forms given to you to be filled out back to the hospital.
What happens on the day of the procedure?
You will be given fasting instructions prior to your admission (usually for 6 hours prior to the procedure). You should bring a list of your medications with you to the hospital. After you are admitted from the admission lounge, your urologist will see you to discuss the surgery. An anaesthetist will see you to discuss the anaesthetic (either general or spinal) before you are taken to the operation theatre. You may be provided with a pair of TED stockings to wear to prevent blood clots from developing and passing into your lungs.
What does the procedure involve?

Figure 2. Penile straightening with penile plication.
Plication of the penis is a procedure where the penis is straightened by bunching up the longer side opposite the plaque by a series of stitches. It is normally used for patients with good erectile function, and curvatures of less than 60°.
It is important to note that the aim of the operation is to make the penis functionally straight to allow sexual intercourse (<15° curvature) so your penis may still have a very slight bend after the procedure.
If you are not circumcised, this will generally need to be done as a part of the procedure to prevent complications and achieve a satisfactory cosmetic outcome.
After a general anaesthetic, you are given some intravenous antibiotics to reduce the chance of infection. A catheter is inserted in your bladder. Local anaesthetic is injected into the base of the penis to relieve discomfort after the operation. During plication of the penis, an artificial erection is created from either injection of a saltwater solution or selected medications. The outer skin of the penis is pulled back (a circumcision is generally performed if not already done). The penis is straightened, and the excess tissue on what had been the outer side of the curve is cinched together by placing a series of stitches or "tucks." The final penile length will depend on the length of the shorter side — the side with the scarring from Peyronie's disease.
An antiseptic solution and a bandage dressing are used to cover the wound. You will stay in hospital overnight. Your catheter will be removed the next morning and you will be discharged with the dressing intact.
Are there any risks or side-effects of penile plication?
Shortening of the penis 80-100%
Mild residual (<15°) curvature of the penis 80-100%
Swelling around the surgical site lasting a few days 80-100%
Permanent altered or reduced sensation in the penis 20-30%
Being able to feel the sutures 20-30%
Minor ooze of the wound 20-30%
Minor infection of the incision requiring antibiotics 5-10%
Severe bleeding or infection needing further surgery 1-2%
Persistence tenderness / discomfort at the surgical site 3-5%
Failure to be completely satisfied with the cosmetic result 3-5%
Erection problems from nerve damage 3-5%
Needing future revision surgery due to persistent / worsening of curvature 3-5%
Major cardiovascular or anaesthetic problems - rare
What should I expect on discharge when I get home?
You will experience some swelling, discomfort and sensitivity at the operative site for a couple of weeks, which should settle with time and with paracetamol and/or ibuprofen. Keep the dressing on for 5 days during which time you should avoid getting the area wet. After 5 days, you can soak the area in water and remove the dressing. You will be given a tube of topical antiseptic gel on discharge, which you should apply to the incision site daily for a week after the dressing comes off. The skin sutures are self-dissolving (takes 2-4 weeks) and do not need to be removed.
After 5-7 days, you can begin light activities again. You should only return to strenuous activity, heavy lifting and driving when you are completely pain free and when your GP is happy with your progress (at least 4 weeks). You should refrain from sexual activity for a minimum of six weeks.
If you develop swelling, fevers or significant pain and redness at the site you should contact your GP.
What follow-up will I need?
You should see your GP in 1-2 weeks for a wound check. Your urologist will see you in the clinic in 8 weeks to check everything has healed well and to ensure you are satisfied with the outcome. No further follow-up is generally needed after this.